Estamos a finales del mes de diciembre de 2019. Se va a acabar otro año. O lo que es lo mismo, vamos a contar otros 365 días y vamos a tener la sensación de que empezamos de nuevo.
Pero no. Todo será nuevo, pero no empezamos de nuevo. Somos los mismos, salvo por aquellos que nos han abandonado, pero no somos lo mismo.
Afortunadamente, en 2019 he hecho cosas que me hacen disfrutar. He viajado por medio mundo, de San Diego a Seúl, de León-Guanajuato a Melbourne, pasando por Londres, Pisa o Kuwait. Todo ello habitando una comunidad centrada en la práctica quirúrgica: #SoMe4Surgery.
Ha sido un magnífico año en el que he conocido sitios y personas únicas, que ayudan a celebrar diariamente que uno vive, además de existir.
Para bien o para mal, tengo nuevas ideas y nuevos proyectos. Algunos son locuras. Otros son sólo experimentación. Algunos están a punto de convertirse en realidad. Veremos hasta dónde puedo llegar. Para ello necesitaré mucha ayuda.
Ever since I can remember, I hate the sound of alarm clocks waking me up. That is why I prefer waking up to a smooth and warm yet artificial light, gradually increasing in intensity like an encroaching daylight. All 365 days of the year, including weekends, the sun rises in my room when the clock strikes 6.30 am. In reality, it is only 5.40 am, because my alarm is always ahead of time. Fifty minutes early; not a minute more, not a minute less, fifty. I am sure that some soft music would never hurt anyone since I sleep alone, by personal choice of course. But then I would have to decide which music would be best to wake up to every morning, and I don’t feel like making more decisions about mundane aspects of my daily life.
If I did not have to go to work, I
would go back to sleep. Otherwise, once I am out of bed I go straight to the
bathroom, always. It is an automatism, completely avolitional. It is the first
thing I do in the morning, an irrational act, just like the rest of humanity. I
undress, empty my bladder, wash my hands, and afterwards look at myself in the
mirror as I attempt to tame my hair, all blonde and tousled, with my damp
hands. At this point in time, I am still fuzzy, whether from sleep or
presbyopia I cannot tell. I stroke my eyebrows, rub my eyes, trace my face with
the tips of my fingers until they rest on my jawline. I don’t know why I do
that, I just do.
I make a living with these hands,
which seem rather common. There’s nothing special about them. From time to
time, I stare at them as if they don’t belong to me. I stretch them out in
front of me and turn them around to look at them from different angles. Five
fingers each, palms and backs, with short nails. I hate the sight of long nails
on a man, and especially on me. I feel a certain disgust when I see them. They
only looked good on de Niro playing Louis Cyphre in New Orleans. “How terrible
is wisdom when it brings no profit to the wise, Johnny”. A feature befitting
the character.
My fingers have been in places other
human beings would consider unusual, not because they are unknown but because
they are nasty. I must confess that it has been pleasurable having them there.
As wide spread adoption of technology has increased in our daily lives, so too has the arsenal of options physicians have to utilize and implement technology to take care of patients. Telemedicine, or the “use of electronic information and communication technologies to provide and support health care,” has resulted in improved access to care, increased resource efficiency, and decreased costs associated with routine health care. Given the promise for this resource, it is expected that the telemedicine market will demonstrate annual growth rates ranging between 20-50% for the foreseeable future.
Surgeons have utilized telemedicine in a variety of ways
over the last decade. Pre- and post-operative patient evaluations utilizing
telemedicine has become common in private practice and academic settings.
Without a doubt, the accomplishments of the US Department of Veterans Affairs
(VA) stands as the most impressive implementation of telemedicine technology. Annual
VA Video Visits exceed more than 1 million regularly, with continued growth and
allotment of resources expected for the next few years. Within the surgical
patient population, the VA has demonstrated safety and feasibility in applying
telemedicine to patients undergoing general, urologic, neurosurgical, plastic,
obstetric, and gynecologic procedures.
When considering new technologies, one must consider all
stake holders and understand the impact that a deviation from the norm may
have. Multiple studies analyzing patient satisfaction, time away from work,
travel time, etc. have shown that patients are pleased with telemedicine encounters
surrounding surgical care. Further, health care systems have demonstrated cost
savings associated with implementation of telemedicine programs. For surgeons,
telemedicine can provide an efficient means of evaluating patients and
coordinating care. As the technology develops, utility in both rural and
metropolitan settings must be assess to identify who would benefit most from these
encounters.
For telemedicine to continue to grow, concerns related to
ethics of the platform must be scrutinized and overcome. The system must
develop in a manner to ensure that health care data breaches are guarded
against such that patients and providers are confident in the privacy and
security of programs. Beyond cyber-security, other barriers hinder the
widespread adoption of telemedicine platforms. First, licensure and practice
laws for health professionals must be adopted that allow surgeons to more
easily interact and take care of patients across state and, eventually,
international borders. Additionally, reimbursement strategies must be
reformatted to allow for patients to be evaluated without physically being in
the same place as their provider. At the national level, enthusiasm for
telemedicine is increasing, and reimbursement related to origination site
requirements and definitions of rural qualifications have been updated to make
telemedicine encounters more broadly applicable.
In conclusion, telemedicine in surgery has received significant
attention as patient satisfaction, decreased wait times, cost saving for both
patients and health care systems have been demonstrated. With an emphasis on
the patient and physician experience, telemedicine stands as an expected and
natural evolution of surgical care. Moving forward, barriers at the local,
regional, and national level must be overcome to allow for widespread
dissemination and implementation of telemedicine in surgery.
Durante
toda mi formación, he escuchado numerosos profesores explicar cómo iba a ser el
siguiente curso, cuáles eran las
dificultades y de qué manera iban a sucederse los acontecimientos hasta que
consiguiera mi plaza en un hospital. Una vez entré a formar parte de un equipo
quirúrgico, hablar de futuro es siempre hablar de incertidumbre. Nadie ha sido
capaz desde entonces de aventurarse a determinar cómo será la medicina de aquí
a cinco o diez años, cómo trabajaremos en los hospitales (incluso si
trabajaremos en ellos) o qué actividad desarrollaremos en los quirófanos.
Sergio Sánchez-Cordero @sesanco – Residente de Cirugía
Actualmente, disponemos de un excelente sistema de salud, tenemos los mejores médicos en formación, los mejores instrumentos y el mejor entrenamiento que hemos tenido nunca, no obstante, las exigencias son mayores y a diario tenemos que manejar con el desequilibrio entre expectativa y realidad de nuestros pacientes. Así como la transformación de la cirugía abierta a la laparoscópica fue traumática para muchos, el futuro próximo revolucionará el marco en el que realizamos nuestra actividad quirúrgica. Por lo que, si una cosa tengo clara es que, la capacidad de adaptación al cambio es la característica más importante de los cirujanos en formación.
Por un lado, la cirugía basada en la
seguridad del paciente y la calidad de vida va a producir un drástico impacto
en la reducción de la iatrogenia en nuestros pacientes. El procesamiento de grandes
cantidades de datos o “big data” y la inteligencia artificial aplicada,
mejorará el conocimiento y monitorizará las consecuencias de nuestras acciones
en los pacientes. Si bien la formación
de los cirujanos estuvo basada en el ensayo-error y el posterior análisis, la
exigencia impuesta por la sociedad, no da margen de error a aquellos que por su
condición de novel tienen más números de equivocarse. Por ello, se crearán
plataformas y simuladores que se convertirán en un peaje durante la formación
del residente.
Si hablamos de innovación y cirugía, el Dr. J
Marescaux, ya explicaba las revoluciones más inmediatas. Por un lado, la
cirugía mínimamente invasiva, definida por plataformas robóticas, cirugía
endoscópica y nuevas herramientas de acción quirúrgica que se están
desarrollando, que hoy en día se encuentran en su expresión inicial, pero que irrumpirán
en los quirófanos del futuro al tiempo que estaremos surcando la cresta de nuestra
profesión. En segundo lugar, la integración y procesamiento de imágenes, tanto
dentro como fuera de quirófano, el procesamiento de imagen a nivel molecular y
la impresión en 3D, mejorarán la visibilidad de aquello que hoy vemos pero que
nos abrirá la puerta a una realidad que actualmente no conocemos.
Y, por último, la revolución social afectará
el modo en que nos relacionamos con el paciente y nuestros compañeros. Las plataformas
digitales e interactivas y los sistemas de “telementoring” facilitarán la
comunicación y la interconectividad entre los diferentes agentes del proceso.
Investigación colaborativa, interacción con los pacientes, congresos online,
etc. son algunas de las aplicaciones que nos encontraremos en un futuro próximo
para beneficiar un mayor número de pacientes.
Por lo tanto, nos encontramos ante una nueva
revolución que cambiará el escenario en el que estamos trabajando. Vienen
épocas inciertas, con nuevos avances y recursos que dibujarán un escenario que,
por ahora, es difícil de pronosticar. Nuestro objetivo como cirujanos es la adaptabilidad
a un paradigma más “tecnológico” en el que seguiremos teniendo pacientes igual
de “humanos”; con el reto de conectar una tecnología cada vez más inteligente y
una humanidad cada vez más incomprensible.
“The best way to predict the future is to create it.”
Abraham Lincoln
Author: Ameera AlHasan, senior surgeon at Jaber Al-Ahmad Hospital, Kuwait
Surgery is an ancient craft that has withstood the test of time thus far. What the tides of the 21st century will bring can only be foretold by examining current trends and using them to steer our profession towards the future we hope to see.
Tweaking techniques through technology
As all aspects of
modern life undergo a rigorous digitalization process, the practice of surgery
is no exception.
Starting with minimally
invasive surgery through the adoption of laparoscopy and robotics, surgical
technology will continue to evolve in order to render operating a more
comfortable experience for both surgeon and patient. The advent of human
enhancement with advanced imaging and artificial intelligence means that the
surgeon of the future will be able to see better and do more.
The improved
understanding of the molecular basis of disease together with the advancement
of nanotechnology has given birth to precision medicine. This novel field
employs targeted therapy to address the subcellular, genetic and molecular
determinants of disease. Speculations arise that this might completely obviate
the need to operate on patients. Although this may be true at certain stages of
a disease, it seems more likely that it will act as an adjunct, leading to a
re-definition of the indications for surgery, and helping to create a multimodal
approach to treatment of which one dimension will remain surgical.
Mending mental and mentorship models
The evolution of
surgery from a mere apprenticeship into a science has led to the emergence of
the “surgeon scientist”, an individual undergoing a metamorphosis from
craftsman into profound thinker, dogma warrior and evidence generator.
As changes
continue to occur in surgical culture and mentality, a dire call is being made
for diversity, inclusivity and equity in surgery. Once this is achieved, it will culminate in
the creation of a melting pot brimming with talent, surgical prowess and
novelty. The naturalization of women into the various fields of surgery is a
leading example of how such inclusivity can capitalize on individual abilities
to enhance overall performance and effect change.
Yet true
revolutions can only be effectively brought about through conscientious
mentorship. Mentorship has been crucial in the formation of surgeons across
centuries, and the future will see a global plea for recruiting more surgical
mentors. This is exactly where communication technology, social media networks
and international associations will play a pivotal role in connecting mentors with
mentees across the world.
Saving the surgical spirit
Finally, the
question we’re all dying to ask is: Will
we continue to operate?
The answer is YES,
because that is what makes us who we are as surgeons.
However, in the
face of technological advances and paradigm shifts, it will be crucial for the
surgical community to foster a kindred spirit in order to continue to operate
and prosper. The surgery of the future will no longer be a one-man/woman show as
focus shifts onto coordinated teamwork and multidisciplinary management.
Successful team
management subsequently beckons for leadership as an indispensible skill for
the thriving surgeon.
The quest has already begun to train and encourage surgeons to become leaders in the future, for the surgical messiah will not be chosen, but created.
Senior surgeons on Twitter who express their interest in becoming #GlobalMentors will be included in the list.
Surgical trainees just need to subscribe and connect with the #SoMe4Surgery mentors in the list.
No matter where in the world they are, trainees will find the right mentor to support their professional development. Mentors will find the right mentee.
With Jeffrey B. Matthews, J ulio Garcia-Aguilar and Richard Hodin: the Boston’s Beth Israel Hospital/Hospital Clinico San Carlos Mentoring team
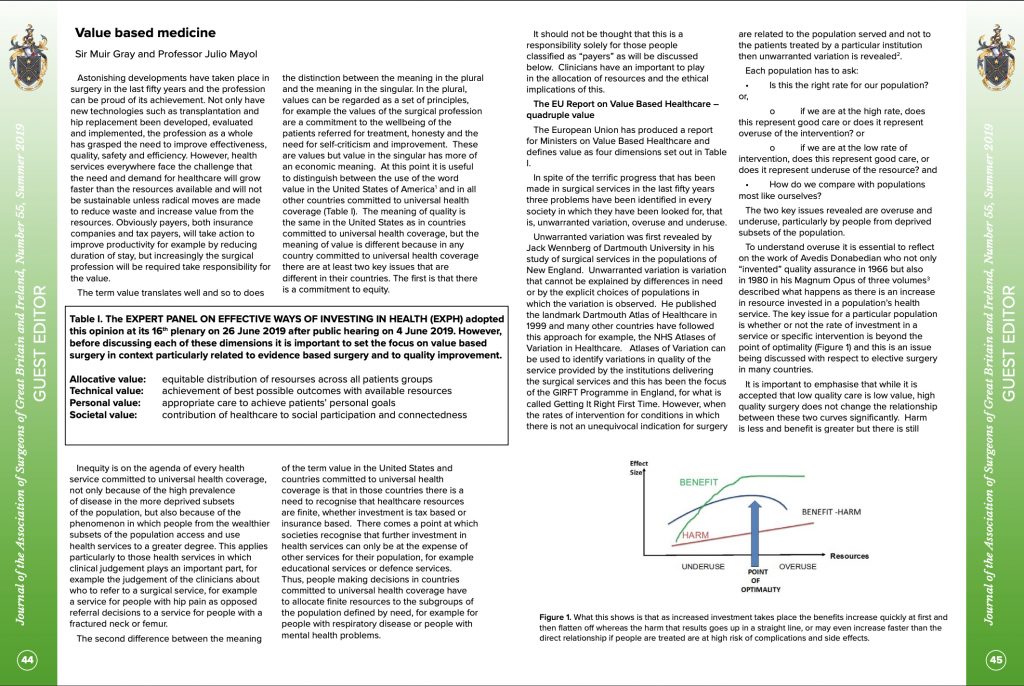
Today, the Association of Surgeons of Great Britain and Ireland has published its Summer 2019 issue, including several contributions around a common topic: Value Based Surgery.
It has been an honour and a privilege to coordinate an outstanding group of surgeons, who have written thoughtful contributions regarding #Telemedicine, #PrecisionSurgery, #DigitalSurgery, #ERAS, and #Outcomes. The list of authors is as follows:
In order to transform the current practice of surgery into #ValuebasedSurgery, surgical leaders must address the following 5 common problems:
Variability in quality and outcomes
Harm
Waste
Inequities and Inequalities
Lack of prevention
Coauthoring an article on #Valuebasedmedicine with Sir Muir Gray was particularly challenging, and funny. Quite an honour, and an unforgettable experience.
Trauma takes numerous lives every year, in both a civilian and military setting. Trauma is the bread and butter of the general surgeon and the humble beginning of every specialized surgeon thereafter. It is therefore imperative to foster a strong online community that brings together efforts to raise awareness, share ideas and ultimately improve trauma practice on a global scale. This is how SoMe4Trauma was born.
Raised under the umbrella of the bigger SoMe4Surgery initiative, SoMe4Trauma aims to breed a community of trauma and acute care surgeons, other medical and non-medical trauma care providers (including ER doctors, nurses, EMS, fire brigade etc.), trauma policy advocates and trauma victims. Some of our goals include connecting the trauma community, sharing tacit & explicit knowledge, advancing trauma education, and creating a friendly and entertaining learning environment. In such a brief time period, the SoMe4Trauma family has managed to grow exponentially and to generate impact on Twitter. Such success can be attributed to a number of factors including the relevance of trauma to the medical community and the public (and the high burden of disease it represents), the unconditional support of influential surgeons on Twitter some of whom are true pioneers of trauma surgery and the continuous interaction of the SoMe4Trauma and SoMe4Surgery members.
Contrary to what it may seem, SoMe4Trauma is not a random tweeting service. The “behind the scenes” work that goes on in preparing most tweets is tremendous. That includes scheduling, networking, emailing guests back and forth, designing posters and recruiting tweeters to help interact and support the conversations. A structured approach is essential as real life efforts get translated into mere tweets. It is our belief that “failing to plan is planning to fail”. Real value can only be generated with vision and vigilance.
Finally, just as management in the trauma bay depends on team work so does the sustenance of an online community like SoMe4Trauma. We invite you not only to interact with us, but to contribute and become a trauma leader yourself. All you have to do is to follow and use the hashtags #SoMe4Trauma and #SoMe4Surgery as SoMe4Trauma continues to blow your mind…hopefully, without causing any injuries 😉
Es posible que todo lo que termine haciendo nuestro cerebro al interpretar la realidad sea lo mismo, y visualicemos cada cosa que hacemos con elementos comunes .
Todo se nos parece a todo. Datos que pasan a información, que pasan a conocimiento, que pasan a ser patrones de comportamiento ante problemas similares (eso que llaman sabiduría). O intuición.
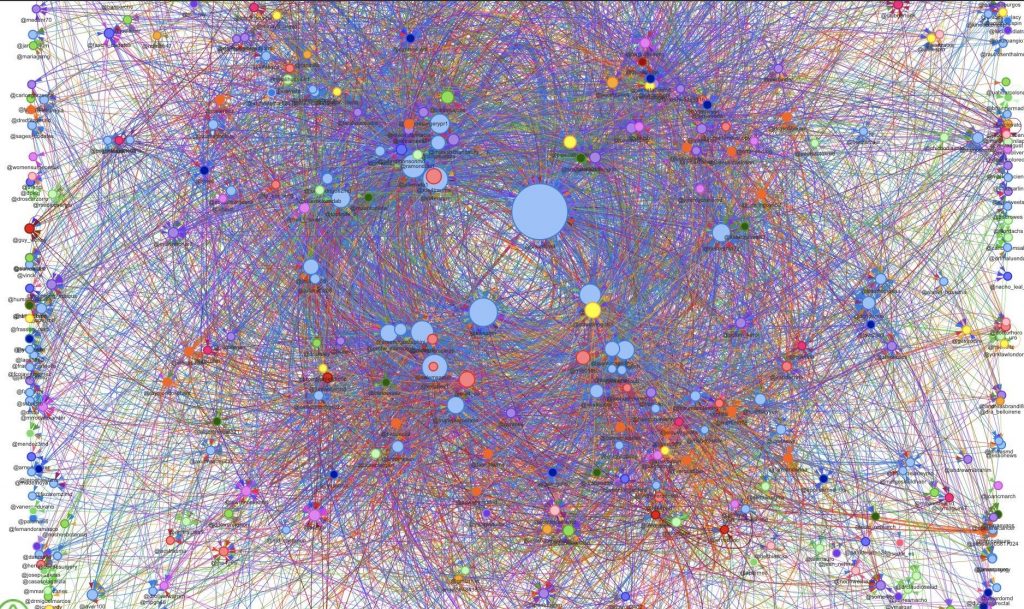
Detalle de las conexiones y flujos de información en Twitter de las 500 cuentas más influyentes que se relación con la mía (punto azul de mayor tamaño). El punto azul más grande y más próximo es Steve Wexner
Cuando hace algo más de diez años comencé a utilizar Twitter, no parecía posible que, en tan poco tiempo, fuésemos a disponer de herramientas para capturar los flujos de información y las conexiones entre cuentas a un coste realmente asequible. No entre dos o tres cuentas, entre cientos de cuentas o miles de cuentas que representan a personas dentro de una plataforma.
Podían ser la representación de neuronas conectadas, podría ser la representación de aeropuertos y vuelos de conexión, o cualquier otra cosa. Pero siempre terminamos representando la realidad de una forma común y análoga. Tendemos a ver la realidad de una determinada manera y a aceptarla en su representación porque es la que nos gusta.
Edinburgh, 8th of June 2019, Prof. O. James Garden retires as chairman of the BJS Society.
Prof. Derek Alderson (left), president of the Royal College of Surgeons, and Prof. James Garden (right)
Looking back, I recall that on the 9th of May 2012, being Prof. O James Garden the honorary secretary of the BJS Society, I was appointed to the editorial board of the BJS. And over the following seven years I have had a meteoric career to become secretary of the BJS Society in June 2018.
Consequently, you might think that what I am about to say is biased, but I must warn you that you would be severely mistaken, because he has been the epitome of a global surgeon long before I even dreamed of becoming part of the BJS community.
Over the last two years, given my role as secretary, I have had the privilege of witnessing his chairmanship of the BJS Society. An extraordinary thinker and strategist, with a strong commitment towards the advancement of our two journals, BJS and BJS Open, and the promotion of global surgical training, James Garden will be deeply missed by all of us in the BJS Executive and Council, but be sure he will always be available if we need him.
Thanks a lot Prof. O.J. Garden. Live long and prosper.